What is cerebral palsy?



We have gathered everything you need to know about cerebral palsy (CP) to make it easy accessible for you.
CP is a lifelong, non-progressive neurological condition affecting a person’s ability to move and maintain balance and posture. It’s the most common diagnosis causing motor disability in childhood, and it usually arises as a result of a combination of events either before, during or after birth. In the long term, people with cerebral palsy are at risk of developing secondary health complication such as misalignments, sedentary lifestyle, lower fitness, fatigue, among others.
The level of severity, and combination of symptoms, differ from person to person depending on the brain injury. Some might only have mild symptoms like a weak hand affecting the ability to write and handle objects. While others might have a severe injury affecting most of the body expressed by little ability to move independently. These people will need 24 hours assistance. Therefore, the available treatment always requires individually adaptation and involvement of different medical and therapeutic specialties.
What is cerebral palsy?

Cerebral palsy (CP) is a permanent non-progressive condition affecting movement and posture. It is often accompanied by spastic muscle stiffness and movement disorders caused by an injury in the developing brain.
It’s the most common diagnosis causing motor disability in childhood and usually arises as a result of a combination of events either before, during or after birth.
What causes cerebral palsy?

CP is caused by an abnormal development of the brain or damage to the developing brain before the age of 2 years. Around 1 in approximately 500 children has CP.
It’s a condition affecting the child’s ability to move, maintain balance and posture, communicate, eat, sleep and learn. CP usually arises from a sequence of events that can cause injury to the developing brain.
Prematurity is the highest risk factor for CP, but it is not necessarily the premature birth itself that causes the disease, but rather a consequence of events that leads to the premature birth that may result in a CP diagnosis. This can be events happening in the uterus while the mother is pregnant.
The specific cause of CP is in most children unknown, but known risk factors that may increase the likelihood of a child being born with CP is:
- Premature birth - Children born before the 37th week of pregnancy
- Low birth weight - This can be children born at term with low birth-weight or a combination of premature birth and low birth weight
- Being born a twin or other multiple birth
- Thrombophilia
- Little oxygen and nutrients to the fetus from the placenta
- Infection of the mother in early pregnancy - This can be different types of viruses, rubella, toxoplasmosis, toxins etc.
- Prolonged loss of oxygen during birth
- Severe jaundice shortly after birth
Is cerebral palsy genetic?
This is a good question. Latest research demonstrates that this may be the case. Scientists have identified mutations in genes that can be responsible for some cases of cerebral palsy. This is not genes inherited from parents but mutations that occur randomly. Further research is needed and is ongoing, and it will give us more insights on this topic in the future.
Can cerebral palsy be prevented?
In most cases, it is not known what exactly has caused cerebral palsy, other than that an injury has occurred in the developing brain. Injuries that occur to the brain during fetal life are usually not something that the pregnant woman are aware of or can prevent from happening. But some risk factors can be reduced in general before and during pregnancy by:
- Making sure you as mother are vaccinated against known diseases, such as rubella.
- Taking good care of your self as mother during pregnancy and avoid alcohol, tobacco and illegal drugs.
- Following prenatal care and seek professional help if she is experience abnormal changes during pregnancy.

How is cerebral palsy diagnosed?

Signs of CP usually appear in early infancy. Visible signs and the degree of signs will differ due to the size and location of the injury in the brain.
Early signs of CP include:
Developmental delays - The child may be slow at reaching expected milestones such as holding the head, rolling over, sitting, crawling, standing, and walking.
Abnormal muscle tone - Body parts are too stiff or floppy. For example, when the child is picked up, the legs get stiff or cross.
Abnormal posture - The child may use one side more than the other and only grabbing toys with one hand, while the other hand is passive or the hand is held in a fist.

Did you know?
CP affects around 17 000 000 people around the world - it is the most common disability in childhood.
It can be very mild, from a weakness in one arm, to severe physical disability, with a total inability to control movements.
What are the different types of cerebral palsy?

CP is typically described according to the main type of movement disorders involved and depending on which areas of the brain is affected. The four main types are :
- Spastic cerebral palsy
- Dyskinetic cerebral palsy
- Ataxic cerebral palsy
- Mix cerebral palsy
Spastic cerebral palsy
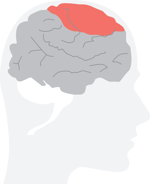
Spastic CP is the most common form of CP, and the damage to the brain is located in the motor cortex. Around 70-80% of people with CP have this type. The symptoms are stiff and tight muscles, which affect the ability of movement. Fast movements of limbs causes increased muscle stiffness. Spastic CP is divided into two subgroups:
- Bilateral CP = both side of the body is affected
- Unilateral CP = one side of the body is affected
Dyskinetic cerebral palsy
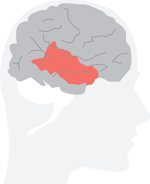
Around 6% have dyskinetic CP which is due to a damage in the basal ganglia of the brain. Typically you will observe variable and involuntary movements.
The movements can be twisting and repetitive and are often described as dystonia. While slow movements are known as athetosis. You may also see more dance-like, irregular and unpredictable movements often described as chorea.
Ataxic cerebral palsy
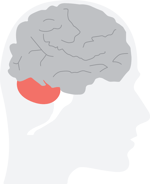
This type is also seen in around 6% of the CP population. This type is related to a damage in cerebellum and is often characterised by shaky or jerky movements and in coordination. The person may also have problems maintaining balance.
Mixed type
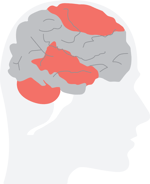
Sometimes a mixed type of the above mentioned types is seen. This is often caused by a combination of damages to the brain in cerebellum, the basal ganglia and the motor cortex.
How is the severity of CP classified?

The severity of the child's motor function skills and communication skills are commonly classified by the use of:
- Gross Motor Function Classification System (GMFCS) – gross motor skills
- Manual Ability Classification System (MACS) – fine motor skills
- Communication Function Classification System (CFCS) – communication skills
Gross Motor Function Classification System (GMFCS)
The GMFCS describes motor performance into five different levels:
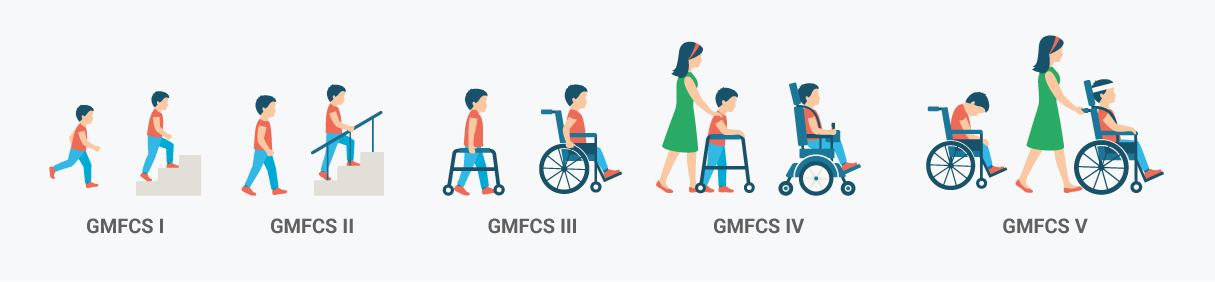
The classification is based on self-initiated movement in sitting, transfer and mobility.The classification contains 5 age bands (under 2 years, 2-4 year, 4-6 years, 6-12 years and 12-18 years). The focus is on which level that best describes the child’s abilities and limitations – “What they do” - based on usual performance in daily life at home, school or in the community.
Each age bracket has its own description level. Here is a description which covers the bracket for children between 6-12 years of age:
GMFCS I – The child can walk at home, school, outdoors and in the community and can climb stairs without the use of a railing.
GMFCS II – The child can walk in most settings and climb stairs holding onto a railing.
GMFCS III – The child can walk using a hand-held mobility device in most indoor settings. He or she may climb stairs holding onto a railing with supervision or assistance.
GMFCS IV – The child uses methods of mobility that require physical assistance or powered mobility in most settings.
GMFCS V – Children are transported in a manuel wheelchair in all settings. Children are limited in their ability to maintain antigravity head and trunk postures and control leg and arm movements.
Read also: What is GMFCS, and why is it used?
Manual Ability Classification System (MACS)
The MACS describes how the child is using its hands to handle objects in daily activities. The classification contains five levels and is based on the child’s self-initiated ability to handle objects and their need for assistance or adaptation to perform manual activities. MACS is suitable for children between 4-18 years of age, while the mini-MACS is for children at 1-4 years of age.
Short description of each level:
MACS I – Handles objects easily and successfully.
MACS II – Handles most objects but with somewhat reduced quality and/or speed of achievement.
MACS III – Handles objects with difficulty; needs help to prepare and/or modify activities.
MACS IV – Handles a limited selection of easily managed objects in adapted situations.
MACS V – Does not handle objects and has severely limited ability to perform even simple actions.

Communication Function Classification System (CFCS)
The CFCS is analogous and complementary to the GMFCS and MACS and also contains five levels describing everyday communication performance:
CFCS I – Effective sender and receiver with unfamiliar and familiar partners.
CFCS II – Effective but slower paced sender and/or receiver with unfamiliar and/or familiar partners.
CFCS III – Effective sender and receiver with familiar partners.
CFCS IV – Inconsistent sender and/or receiver with familiar partners.
CFCS V – Seldom effective sender and receiver even with familiar partners.
How does cerebral palsy affect people?

CP is a condition affecting a person’s ability to move, maintain balance and posture, communicate, eat, sleep and learn. The severity of the CP differs from person to person depending on the brain injury. Some may only have small symptoms like a weak hand affecting the ability to write and handle objects, while others might have a severe injury affecting the whole body and all functions. This person might be in need of 24 hours assistance.
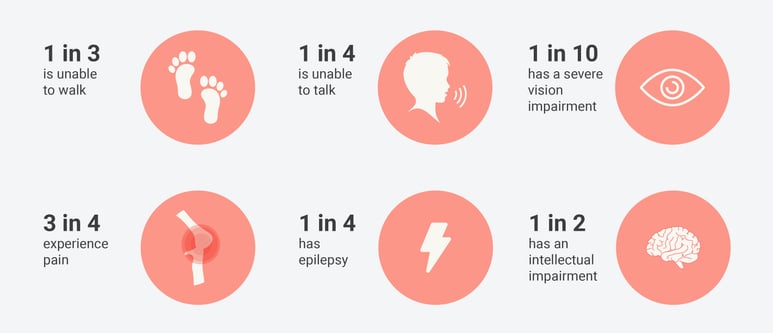
From extended research on people with CP we know that:
- 1 in 3 is unable to walk
- 1 in 4 is unable to talk
- 1 in 10 has a severe vision impairment
- 3 in 4 experience pain
- 1 in 4 has epilepsy
- 1 in 2 has an intellectual impairment
What kind of treatment is available for people with cerebral palsy?

Unfortunately, there is no cure for CP. However, there is good evidence that different types of intervention can improve function, capabilities and prevent secondary complication related to the diagnosis.
Treatment of people with CP requires a multidisciplinary team of professionals, such as medical doctors with different specialities, physiotherapist, occupational therapist, speech therapist, neuropsychologist etc.
A physiotherapist and occupational therapist will support the child and the family in functional training and will use different approaches and evidence-based methods. It is well documented that it is important to set functional goals that matters for the child and the family. This to produce motivation and progress. Sometimes the child is not able to identify goals by itself, but then goals should be discussed with parents. Therapists will help families in setting realistic goals in relation to the child’s ability and make sure the goals are challenging but achievable.
It is recommended to directly work on the goal for the child. For example, if the child wants to learn to ride a bike, then the training should include bicycling. To make training motivating, it has to be enjoyable for the child. If the child is crying or stressed it is not a good learning environment.

Read also: Why Is Early Childhood Intervention so Important?
Functional training should as much as possible be carried out in a real-life environment, like the child’s home, kindergarten, school or playground. If this is not possible, we should try to adapt the environment to simulate a real-life situation for the child.
To achieve functional skills often requires a high dose of training, and the training is often a combination of eye-to-eye contact with a therapist and the training carried out by parents. Therapists will educate and guide parents to empower the family to carry out training during daily life and implement training in daily tasks.
This to be able to achieve a high enough dose of training to be able to reach the goals. It takes approximately 14 hours to learn a new skill and around 40 hours to improve a skill. Therefore, it is important that goals are realistic also in terms of time available for training. So, time and resource availability in the individual family should be taken into consideration when setting goals.
Therapists and doctors will together with the family identify factors that are limiting goal achievement.
That may be limitation related to range of motion in joints or high degree of spasticity.
Spasticity can cause pain or limitations related to positioning in sitting and standing. Different treatment option for muscle spasticity treatment is available, such as:
- Botulinum toxin – medication injected into muscles, typically in limbs, inducing temporary reduction in muscle tone. This treatment goes hand in hand with conventional treatment such as physiotherapy, to improve function.
- Baclofen – medication supplied either orally or through a pump and gives spasticity reduction. Medication through a pump is often more effective, because it is delivered right where it is needed and at a lower dose. Placement of the pump is a surgical procedure.
- Selective dorsal rhizotomy surgery (SDR) – involves sectioning of some of the sensory nerve fibers that comes from the muscles and enter the spinal cord
Orthopaedic surgery, either on muscles or joints, may also be needed at some point in the child’s life or when growing into adulthood. This intervention aims to optimise function and prevent deformities.
Several countries have introduced follow-up surveillance programs for people with CP with the aim of:
- Preventing hip dislocation and severe deformities
- Gaining knowledge about CP
- Improving cooperation between professionals
These programs monitor people with CP from infancy to adulthood with regular assessments. Assessments includes measurement of joint range of motion, spasticity and X-ray of hips. In addition, treatments, surgeries, use of orthosis etc. is recorded. The continuous and standardized monitoring enables early detection and deterioration and creates conditions for preventive treatment at an early age.

How can assistive technology compensate for the disability?
.webp?width=300&name=Device_small%20(1).webp)
Assistive technology is any device or piece of equipment that can compensate for impaired motor function and thereby enable a person’s independence and participation in everyday life. It can be devices for mobility, eating, participation in activities, learning, hearing, communication among others .
The need of assistive devices will vary depending on the person’s age, functional ability and capacity. Also, the environment the person is living in, and the level of assistance needed, will influence type and numbers of devices the person may need.
Mobility Equipment
Most people with CP will at some stage in their lives be in need of a mobility device. This includes both walking and wheelchair technology.
Walking Aids
Walking sticks and crutches – different options are available, such as quad or tripod base sticks, elbow, forearm, gutter and axillary crutches.
Walkers – these hand-held walkers can be posterior walkers, where the person uses the walker behind them or an anterior walker, where the walker is in front the user. The walkers can have up to 4 wheels.
Gait trainers – Gait trainers typically provide more support at the level of trunk and pelvis compared to hand-held walkers, and they often also have options for head support.

Read also: All for Ella - and an independent life despite of her CP
Wheelchairs
Manual wheelchairs – these chairs can be propelled by the user or pushed by an assisting person. They may be light chairs with little support, or more comfortable chairs with the option of reclination.
Powered wheelchairs – powered wheelchairs are motorized and allow the person to control mobility on their own. These chairs are available for very small children and up to adults. They come with many different features and options.
Wheelchairs are available for both indoor and outdoor use.
Devices for postural support
Standing frames – for those who are not able to stand or walk on their own it is recommended to use a standing frame on a daily basis. Several different options are available such as: sit-to-stand, prone, supine and multi-position standers, mobile standers and dynamic standers. Dynamic standers like the Innowalk allow even people with severe disabilities to move both legs and arms while standing with weight-bearing.
Read also: [Video] Ada Has CP – This Is Her Experience with the Innowalk
Seating Systems – supportive seating comes in many different set-ups, but the aim is to support the person in an appropriate position to increase balance, activity and participation.
Sleep Systems – supportive positioning equipment used to increase comfort for a person in lying, including cushions, rolls, wedges, mattresses etc.
Daily activity aids
These are devices to accommodate activities of daily living such as:
- Toileting – raised or lowered toilet seat, benches etc.
- Bathing – adapted bathing tub, shower, non-slip mats etc.
- Eating – adapted cups, bowls, plates, spoons, forks, knives etc.
- Beds – adapted beds with different features to ensure safety and comfort.
Environmental adaptations
Environmental adaptations are used to limit or remove barriers in the home, nursery, school, workplace etc. to promote independence and reduce the burden on caregivers. Here are some examples of modifications:
- Automatic door opener
- Ramps
- Threshold eliminator
- Through-floor lift
- Hoist
- Grab bars
- Adaptable height on kitchen table, bathroom sink
Equipment for recreation or sports activities
People with CP are less physically active compared to typically developing people. Assistive devices allow people with a disability to explore and be active, participate and interact with other people. Devices for such purpose may be:
- Bicycles or Trikes
- Race runners
In addition, several sporting activities can be adapted to allow people with disability to participate.
Orthotic devices
Orthotic devices are braces made for the individual person to improve function and strength. Orthosis are available in rigid, dynamic or soft forms and are prescribed by a therapist. Orthotics can include:
- Knee/Ankle/Foot orthosis
- Arm or hand orthosis
- Spinal orthosis
- Lycra suit
Communication technology
Many people with CP struggle with communication, but technology within these fields have been amazing, and today several types of devices are available to improve communication. Devices may be:
Communication boards - a type of augmentative and alternative communication device. It has symbols for activities, tasks, feelings etc.
Speech generating devices – an electronic augmentative and alternative communication system that can supplement or replace speech or writing for people with limited ability to speak.
Eye-tracking devices – allows a person to use their eyes to operate a computer or tablet for communication.
The list of assistive devices mentioned here is not complete, and availability and reimbursement will differ from country to country.
A multidisciplinary team will support each child or adult in finding the best available equipment to support function and enhance independency.
What is the life expectancy in people with CP?

There has been no general studies of life expectancy in people with CP, but most people with CP live between 30-70 years.
